
The Healthcare Breakdown No. 064 - Breaking down Physician pay, hospital subsidies, and the path to renewing the pipeline
Brought to you by questioning your life decisions when you see what they pay a manager at Buc-ees

What we’re breaking down: Physician salary, debt, and health system subsidies
Why it matters: These dynamics are making healthcare less accessible, less independent, and more expensive (you’re shocked, I know)
Read time: The last 6 minutes of your drive back from the lake last weekend that took 86 minutes (7 minutes for real though)
Oh, hi. Missed you too.
I thought it might be nice, since we haven’t seen each other in a while and you are enjoying that lovely mimosa to talk about why all our awesome doctors seem like they are riding the express lane to health system employment. And because of that, why it’s hard for independent practices to hire those bright-eyed bushy tailed newly minted physicians.
You may also know that I have this thing about independent physicians. About happy physicians. About patients getting the care they deserve and allowing their doctors to truly be in charge of that care.
Call me a hopeless romantic.
Here’s a chart we all know and don’t really love:
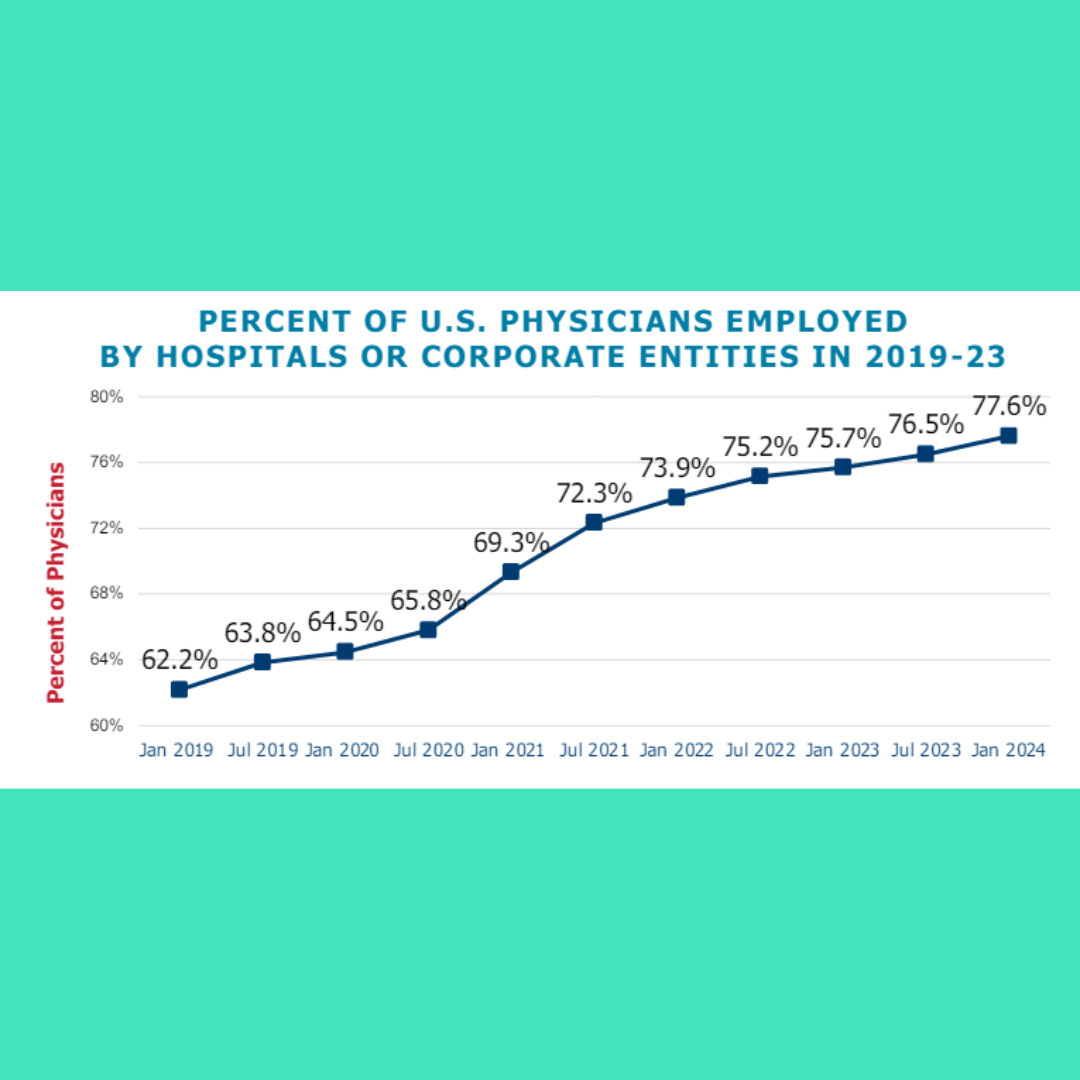
The question is why? Why are we seeing employment continue to rise?
Another question is what does that mean for the profession overall and specifically my dudes in independent practice?
Most importantly, what are we supposed to do about it?
Well I have some ideas on all of the above since I’ve been at the dock of the bay for the last four months, thinking about this moment. So, let’s get into it.
First, why?
There are a couple of reasons, three big ones in my opinion.
1. The pipeline
Let’s do some fun math real quick. It’s why you’re here after all. That, the jolly humor, and to make a drinking game out of spotting grammatical errors.
Layup.
This is for my cardiology friends out there holding it down.
Between medical school, residency, and fellowship, a cardiologist is about 10 years deep past undergrad and has a fat negative bank balance of about $331,000 according to a random statistic I found on the internet.
Now, the good news is according to some other random internet facts the national average salary of a cardiologist is about $525,000.
Solid.
While that salary is nice, don’t forget all that debt to carry.
I also want to pause here before any of you out there dutifully reading about to decry the amount of money a doctor makes, may I just remind you that physician pay only represents about 9% of total healthcare spending.
Also, consider that these people literally save lives everyday, so the value tradeoff definitely seems to be there.
Sorry, tangent concluded. Don’t come at me.
If we play out the debt equation on a standard, non-refinanced loan at 6.8%, this genial cardiologist is on the hook for about $690,000 in total loan payments over the course of about 25 years.
Just think about that for a minute.
That’s a lot of quiche. And sure, she may be earning a lot, but paying over 2x a loan amount, trying to also make up for the income you had to forgo for 10 years is a deep hole to climb out of.
Not to mention that workload, admin load, moral injury load, and generally the load that our physicians take on a daily basis.
Here’s the kicker. This scenario plays out differently in different settings.
While this scenario may be true in private practice, or a large medical group, things change if you look into the non-profit sector.
Certain positions in large non-profit institutions may also come with loan forgiveness. Whether in the form of signing bonuses, stay bonuses, direct loan forgiveness, or eligibility for Public Service Loan Forgiveness. And while you may not make as much on an annual basis, total payments before loan forgiveness may be as low as $120,000.
That’s a $570,000 difference in payments and decades of time off a loan term.
So, just imagine, you have been grinding for 10 years at one hospital, staring down the barrel of nearly $700K and 25 years of payments, and that hospital sits you down and offers a sweet deal worth over a half a million dollars. What are you gonna do?
Not just that, what options do you think you have?
Because realistically, if you turn to the private practice route, there just isn’t necessarily the same scrooge McDuck money vault swimming pool filled with 340B, private equity, facility fee, and uncontrollable contract rates allowing them to subsidize these a $525,000+ salary, knowing how much return they will be able to make off a single specialist in their system.
Spoiler, it’s about 6x.
If you weren’t defeated enough (I know it’s kinda my thing), let’s move on to the next reason.
2. Insurance is effing around and finding out
All right, let’s give our poor fresh fellows a break. What else is drives the employment model?
Insurance. Duh. It’s always insurance.
When a company can unilaterally control the fees paid to a physician practice and predicates those rates on size, where does that leave most independent practices?
At the mercy of 100% Medicare rates from 5 years ago. And in some cases, 85%. Thank you sir may I have another.
We will leave this discussion for another issue, but know that this unfounded leverage strategy makes no practical sense other than to help line the processors’ pockets and help drive consolidation.
And finally!
3. The exit
Here’s another big one. Imagine you have worked for 30 years, building your practice and feel like you are ready to finally take that trip to Italy you have always dreamed of. But that Lake Como life costs $4,000 a night.
Listen, I am all about wandering around the Italian country side finding a passable hotel with 2 stars, hoping they have a room, and then toughing out the lack of air-conditioning taking turns with you buddy Dave for who has the bed that night, but sometimes you gotta treat yourself.
Not to mention that after that trip, you want to slow down and maybe think about riding off into the sunset of retirement.
So the question becomes: who’s buying?
Your junior partners? How much money do they have? Do they want to run a business? Do they know how?
The health system? They have the vault and all…
Barron and his dad’s private equity group? Everyone hates them, but they’re also cutting 10x EBITDA checks.
These are real issues all reshaping the dynamics of healthcare delivery. All with different calculations, earnouts, restrictions, preferences, requirements, and side effects. But you better believe that it is going to be hard for anyone to turn down the “big payday” from PE or from a health system.
That too is a discussion for another day, as there are about 39 ways they will make the deal look really good and somehow your $10M payday turns into $1.5M. And sometimes your $1M payday turns into you owing money.
Seent it.
Knowing there may be less upside based on loans, instability from being at the mercy or insurance, and a potentially limited long-term path to ownership, it’s not much of a wonder as to why the pipeline is dry.
Okay Debbie downer, what then? Because it seems like the pipeline is broken, not just dry. And even if you do go that route, it still seems like all roads lead back to consolidation.
So glad you asked, thank you. I knew I liked you.
Let’s back it up to the health system.
How do they get that juicy 6x return on salary? Sure, it’s the direct contribution of the physician and making most of your money on facility fees. But it’s all the other things they can make as a result of having a patient stay in their system. MRI, CT scans, procedures, drugs, and yes, more facility fees.
All the dollar signs.
The issue is we have been playing the wrong game.
The game isn’t salary. The game is ownership.
The path is building something.
It’s easy, and don’t get me wrong, important, to talk about, fight for, yell into the void about reimbursement.
But the bigger opportunity and what is going to move the needle is ownership.
Own the ASC. Own the OBL. Own the imaging equipment.
Participate in the fees where CMS and processors are paying the most. Direct contract. Get into value based arrangements after you are positioned to own as much of the continuum for the patient as possible.
Rheumatologist should provide infusions. Ortho, interventional cardiology, urology, go get involved in an ASC. Build one. Invest in one.
Find a physician owned hospital and get in there.
Hospitals and private equity play the game. They own as much as possible.
Now that I have type ranted a little, let’s go back to the pipeline, because realistically ownership isn’t easy. It’s hard, but the payoff is worth it.
But even if you buy it, we are still missing a couple of key ingredients. Like pizza without the sauce and cheese. Bread, that’s just bread.
First, it’s the education. They don’t teach you business in medical school. They don’t teach it in residency. And they definitely don’t teach it in fellowship. In fact, I would argue that it is detrimental to hospitals to have their doctors exposed to business.
Why?
Because then physicians could see that they are getting a short term, decent deal, but long-term raw deal. That the hospital is profiting disproportionately off of their hard work.
Remember: no doctor, no reimbursement. No facility fee. No contract rates.
And big love to every clinician on the team making it happen.
Second, they don’t get shown the outcomes. That at the end of a 30 year career, one which you were in charge of, owned your patient relationship the whole time and unequivocally, were in control of your time, and at the end owned several valuable assets.
We don’t see that outcome enough. But it is out there.
The flip side of that? The worst case scenario… the health system never stops hiring doctors.
So, yes, we have a people problem in healthcare. But really it’s a math problem. Large institution employment makes healthcare more expensive and less accessible.
Independent ownership, makes it less expensive and more accessible.
It’s up to us to show the pathway and the upside.
See you next time!
Here’s what I just said in one sentence: The current financial incentives and economic realities make employment more appealing, while undermining the long-term viability of the practice of medicine. The path forward is physician ownership and better pathways towards that end.
Sorry, for the extra sentence.
It felt important though.
Love you.
I think you'll appreciate this highly related post https://substack.com/home/post/p-172872769
I love your breakdowns. You make it so simple to understand and sound so easy to do…then the real world smacks us in the face and says “HA!” I’m going to add a bunch of bureaucratic nonsense to make things interesting. Unfortunately, not many people want to wade through the nonsense. (I guess that is what gives those of us in consulting a purpose?!)
Thank you, as always, for your words of wisdom.