
The Healthcare Breakdown No. 018 - Breaking down MedTech Part I: The playas
Brought to you by my cousin’s failed hip implant

What we’re breaking down: All things MedTech in this rousing 3 parter
What you’ll learn: All kinds of stuff
Why it matters: MedTech is an 800 lb. gorilla in healthcare, that not many people seem to talk about. I think we should.
Read time: Sometime before tomorrow (10 minutes for real though)
This issue is sponsored by MedTech Militia.
Check out the awesome logo:

MedTech Militia is a community of MedTech innovators and all about that value.
Here’s some of that value you can expect:
1:1 virtual coffee with VPs of sales, founders, and all-around great folks.
Onboarding meeting with the founding team of veteran MedTech gurus.
Learning from community members with probably like 793 years of combined experience.
Resources to help you grow and thrive in MedTech.
Career development like you’ve never seen it before.
Really nice sports coats.
And so, so, so, much more. Like, promise. It’s going to be awesome.
Check it out at: medtechmilitia.com
Back to the show!
All righty. You may not know this, but I spent a few years in the old MedTech space. Back when they still just called it medical device. No cap.
Like, no capital letters. I don’t speak the kids’ lingo.
The difference, if there is any these days, deserves a brief explanation.
MedTech refers to the modern era, more high tech stuff in medical devices.
Medical device is the catchall and would include things like sutures and wound dressings. I know, wouldn’t think it, but it does.
Out of respect for the aforementioned militia, I am going to refer to everything as medtech in this series. I will however, not be capitalizing it. Way too much keyboard effort.
MedTech also sounds cooler.
Ok, enough stalling! Onto the meat.
MedTech Part I: The playas!
In what hopes to be an interesting series, I am going to dive into the world of medtech. To start, we have to get to know the players critical to making this thing go round. If we don’t, then who ever would be able to make heads or tails of tracing fees, tiered pricing, rebates, and all the other billions of fees?
See, gotta know the game. Well, the players in the game.
There’re 4 big ones. 5 if you include payors, but we are going to leave them out for now and may have a special episode dedicated to that nonsense another time.
Here they are:
MedTech companies (duh)
Hospitals, in 3 flavors
Distributors
GPOs
1. MedTech companies
These would be the good people making devices. Think Medtronic, Boston Scientific, Siemens, Baxter, Stryker, GE Healthcare, Johnson & Johnson, Philips, and a whole bunch more that don’t make billions each year.
These businesses are relatively straight forward. Mostly companies are selling goods with some services on the side depending on the company.
Part II is going to be a deep dive into the medtech company, so I won’t spend too long here.
For a good understanding of a classic medtech company, you need look no further than its income statement.
Here’s Boston Scientific’s:
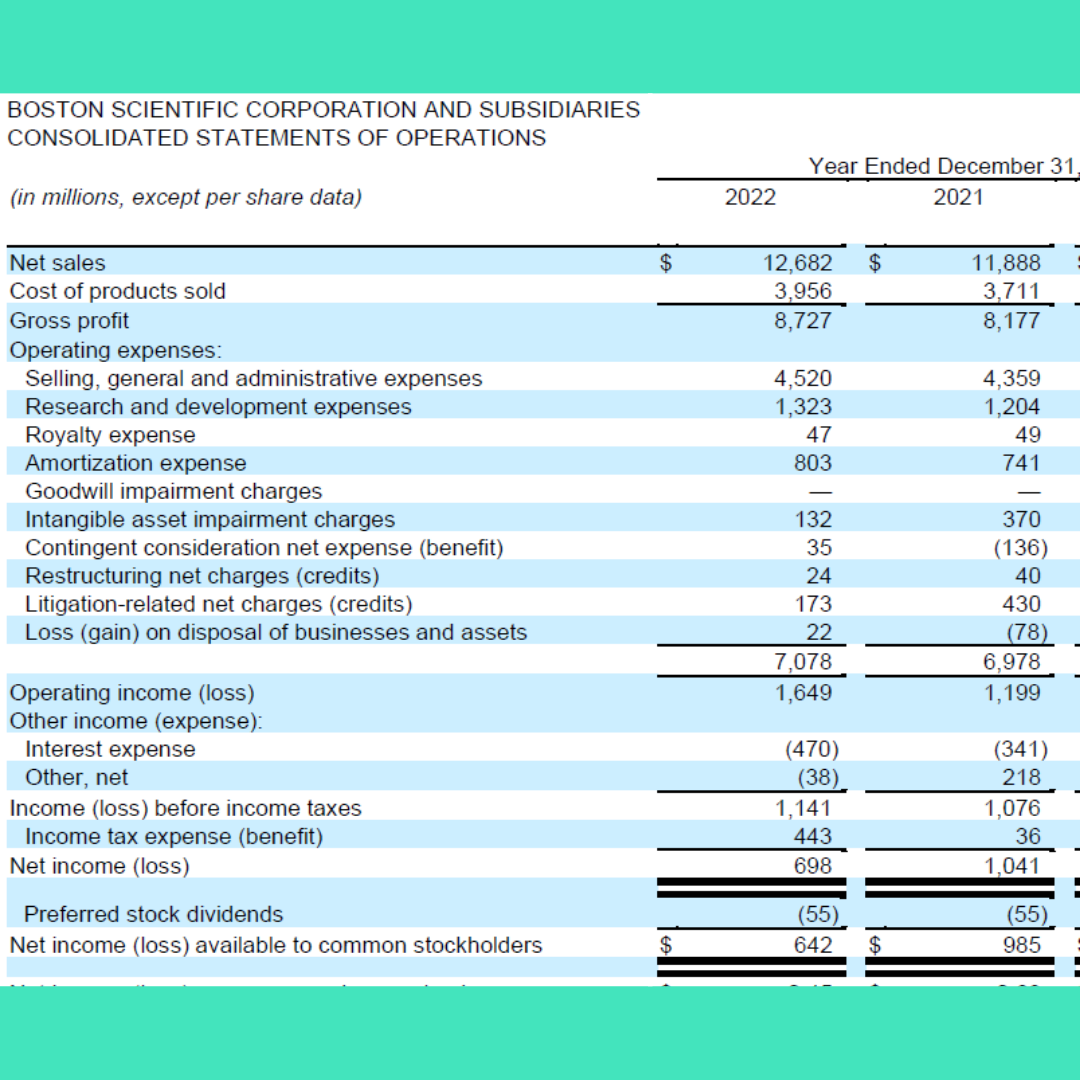
As you can see, fairly straightforward from a high level. They make things and sell things.
In their own words:
Translation: We make stuff. We sell that stuff. We’re awesome.
As you can also see, there are 3 main buckets of expenses:

Cost of Goods Sold – 31.2% of net sales
Selling, General, and Administrative – 35.6% of net sales
Research and Development – 10.4% of net sales
Now you can very easily see the levers the company has to pull, to lower expenses and drive profitability.
Well, there is one other lever. A very important one in the context of healthcare’s ballooning costs.
That is, price.
Medtech companies can cut costs or raise prices.
Cutting costs is hard. If you really want to get granular the two biggest costs after cost of goods are sales and marketing.
Those are also the revenue engines.
So companies will try to get operationally more efficient, but that’s also a real pain in the tush.
Low hanging fruit? Raise prices.
Or pass on costs. We’ll go over each of these moves in Part II.
For now, on to the next player.
2. Hospitals
If you thought this one was going to be simple, you’d be wrong.
There are three main types of hospitals. At least from the medtech perspective.
A hospital, stand alone. Doing it’s own thing. No system, just chilling. Like Grady in Atlanta.
Health systems – This term covers all manner of sin. You may have also heard of an Integrated Delivery Network or IDN. An IDN is a type of health system. The particulars aren’t that important. There’s some different types, but just think of a bucket load of hospitals and other care delivery settings under one name. Like Mayo. Not the bread kind.
Aggregate groups – There is some cross over here with GPOs, so I will mention it there as well. This is a crew of health systems that ride together to get better pricing, terms, the whole thing. Pooling power to negotiate.
So, not totally simple, but simple in the way that this is the customer. We, the medtech mafia.. wait, scratch that. That feels incriminating.
We, the good upstanding medtech folks of the world, want to sell as much of our stuff as possible to customers. Those guys up there.
The key thing to note for this player is there are two things they care about. Sorry, not sorry.
Cost and outcomes.
In that order.
But there is a caveat. A big one. Cost is relative to a lot of other things going on in the world. Something you will come to see as you dutifully read all the parts in this series.
I’ll give you a quick teaser.
Say you come up with a really cool idea to say, make a device slightly better and 20% cheaper. You call the hospital. They ask, “what GPO are you on?”
Huh? Fine, call the GPO. They ask, “well, how many hospitals are you selling to?”
Rats. Chickens. And eggs.
Cost savings is important. Outcomes means a lot of things. Physician preference barely exists anymore.
The prevailing reality is that unless you are a big medtech player, you’ll mostly be treading water. Some exceptions apply.
But first! The next homie.
3. Distributors
Cool. You’re a medtech company. You have a product, or like 800 products. How do they get to customers?
Well, UPS is an option. So is FedEx. But more likely you are going to use a distributor.
The likes of McKesson, Cardinal, Medline, Owens and Minor, or maybe even Henry Schein.
These guys work on volume and the thinnest margins in town. You thought hospital margins we anemic.
Check McKesson:

Revenue: $277B
Net profit: $3.56B, 1.29%
I mean, I’d take $3.56B for sure. I played the lottery the other day and that was only $1B.
Why are margins so thin? The life of a distributor.
Here’s the skinny. Medtech companies sell to hospitals. McKesson, though it has a whole host of products and services these days, is the box mover. It makes money (from a distributor perspective) on fees. And you can only charge so much in fees.
Fees the hospital pays to have the honor of it as a distribution partner. And fees the medtech company pays to know where the distributor has moved its product.
These are also known as tracing fees.
Head spinning yet? Well, buckle up.
Just because I “sell” a product to a hospital, doesn’t mean the hospital buys it from me. Often, it will buy from the distributor. The hospital buys at a price I set, but goes to the distributor. Because the distributor bought from me at a higher price (distributor or list price), I then give the distributor a rebate for the difference in price it paid from what the customer paid. Then I pay the distributor to tell me who bought, at what price, and how much (tracings).
I know. I knowwwww.
I made a picture:

The takeaway when we tie everything together is the money. It’s always about the money.
Do you think a Medtech company is going to just eat the fees it pays to the distributor? Exactly. I don’t eat broccoli just because it’s good for me. I do it because my daughter makes me.
Distributors realized they weren’t making hay on such meager fees. It’s why most distributors now make and sell products as well. They want a piece of that medtech margin.
And it’s working. They’re still mostly in the disposable commodity business, but who knows what’s on the horizon.
Oh, also worth noting that large medtech companies do sell direct. Small ones do too. But most large health systems prefer to go through distribution. It’s like ordering from Uber eats instead of calling 7 different restaurants because your significant other likes the fries from one place but the burger from another. Streamline.
Ok, so we have medtech companies selling stuff to hospitals and distributors moving the boxes.
That leaves one mainstay, the Group Purchasing Organization.
4. Group Purchasing Organizations (GPOs)
I get it. This is getting long. But I swear, we’re almost done. Then you can refill the mimosa you finished 17 minutes ago. It’ll be worth it. Promise.
Way back in the good old days, medtech companies had the upper hand. They could charge whatever they wanted. How could a paltry 250 bed hospital hope to negotiate with Medtronic?
It couldn’t. So, that little old hospital called 98 of its hospital buddies to pool buying power. Bad boys for life.
There are 3 major GPOs in medtech land.
Prermier, Vizient, and HPG.
HPG is also known as Health Trust. It’s owned by HCA. Fun fact.
Some other large health systems have followed suit and created their own GPOs. One example is Northwell, formerly, Northshore LIJ.
GPOs are super fun. Here’s how they work.
Each represents thousands of hospitals. If you want to sell to a hospital, you often need to go through a GPO.
Why? Because GPOs hook up hospitals based on their compliance. Meaning, the more a hospital buys from the GPO, the more money they save.
To have the honor of buying from a GPO, a hospital pays fees. Ya, fees again. It’s a wonder healthcare is so expensive.
And, if you are an eager medtech company, you also pay fees for the honor of being on a GPO contract. You pay based on sales. Usually around 3%. Sometimes 2% if Chris Voss taught you how to negotiate.
To further confuse you, GPOs have categories and tiers. For example, surgical gloves may be a category. There are two suppliers (dual-source) on your GPO for that category. If you spend less than $100K annually, your price is X and you are on tier 1. If you buy more you go up in tier and down in price.
These days there are like 6 tiers and super double secret tiers.
It’s a give and take game on the part of the medtech companies and GPOs to try and be as sticky as possible.
For example, I will create a double secret probation tier but the hospital has to buy 90% of that category from me and it will get the best pricing in the world. The GPO is happy because the more the hospital spends “on contract,” the more the GPO makes.
And the more the hospital spends “on contract,” the more the hospital saves.
In theory. Did you know that hospitals actually save more off contract than on. Ya, they don’t tell you that much. It’s true though. But we’ve always done it the other way, so…
To round this out, remember aggregate groups? These are like crews of crews on GPO. Some hospital really wants that double secret tier, but just isn’t big enough for the spend. What do they do? They call up their bigger buddies and make an aggregate group so they can all relish in their higher tier position.
Like inception for buying groups. Buying groups within buying groups. The deeper you go, the more likely you are to go insane.
The relevance to medtech? Well, you saw that SG&A number. Medtech companies can’t get by with run of the mill sales teams anymore. They need corporate account managers, national account managers, GPO contract specialists and executives, and more.
How do you cover all those costs? You guessed it. Popsicle sales. No, wait, raise prices.
Mkay. That’s it for today. I am going to go curl up in a ball and cry.
Hope you enjoyed Part I of the medtech takeover: the playas.
Next week, the insiders look at medtech.
Don’t miss out.
Love you.
Preston, this segment of health care has been incredibly difficult for me to understand. I see many small medical equipment companies around town and often wonder how each survives. Each one sucks at customer service. Each one has terrible processes. After you are done engaging with each entity, you throw your arms up in frustration and wonder what you have actually accomplished.