
The Healthcare Breakdown No. 034 - Breaking down the great game of horse trading in healthcare… and pie
Brought to you by the year of the horse

What we’re breaking down: How the game really works in healthcare, all of it
Why it matters: The pie isn’t going to shrink anytime soon, we need to be ready for that
Read time: Die Hard runtime, which is much longer than the actual runtime since you’ll rewind the best scenes at least ten times (7 minutes for real though)
If you grew up in the age of writing papers by hand or maybe even on your handy dandy word processor, you’ll fondly remember trying to hit that mythical page minimum to impress your English teacher.
Nothing cries “A-” like a clean 5-page double spaced masterpiece on the imagery in a Jack London essay about wandering in the snow. And to sprinkle fairy dust on the accomplishment, you’ll want to embellish your prose with a hefty use of idioms, metaphor, analogies, and maybe even the occasional alliteration.
What does this have to do with anything? Well, other than doing an excellent job of unnecessarily lengthening this episode, just like your Earnest Hemmingway paper, we use a lot of analogies and such in healthcare.
The two for today’s theme are pie and horse trading.
Let’s start from a macro perspective. I’m sure you saw it, CMS just released the latest US healthcare spend number.
$4.5T.
For context, the top three economies in the world are, in order:
The United States - $25.5T
China - $18T
Japan - $4.2T
We spend more on healthcare than Japan’s entire GDP.
Party.
So, what’s the deal. Why can’t we make that dang number come down!?!?
Well, why would we?
Because other than representing costs on one side of the equation, on the other side it represents jobs.
While we could, do, and should make good arguments that a significant portion of those dollars is going to line a select few pockets, is being spent in other countries, shouldn’t be that high from waste, etc. the fact remains that it is a direct reflection of jobs in the country.
The master of ceremonies in healthcare, UnitedHealth Group for example, employs 440,000 people, roughly.
Should UHG exist in it’s current form? No.
But who is going to make it obsolete and eliminate 440,000 jobs?
We can talk about disruption, innovation, all that great stuff, but you know who definitely isn’t going to do anything about it?
The government.
Joe can’t run a campaign on a shrinking GDP and job decline. That’s what real healthcare regulation would do. It’s what it should do.
So, you can see how the stage is set. The whole literal government not exactly lining up to reduce healthcare spending because of the impact on jobs.
On the other side of that coin, you have massive companies. Five of those companies employ dang near 1 million people and earn almost $1T of the $4.5T, not to mention the rest of the global players from large health systems to medical device companies, pharma, and all the dainty middlemen literally in between.
When the healthcare pie shrinks, their revenue goes down. When their revenue goes down, so does their stock. And everyone seems to think that the stock market is a direct reflection of the economy. It isn’t, but we can talk about that another day.
Cool. Well, not cool, but here we are.
There is no single interest (other than the American people that is) who are really, actually interested in lowering the cost of healthcare.
Since the pie isn’t getting any smaller, it’s left to the prevailing organizations to figure out ways to maximize their returns. To achieve these ends, they largely engage in horse trading hijinks. Pushing the circumference out, while growing their piece.
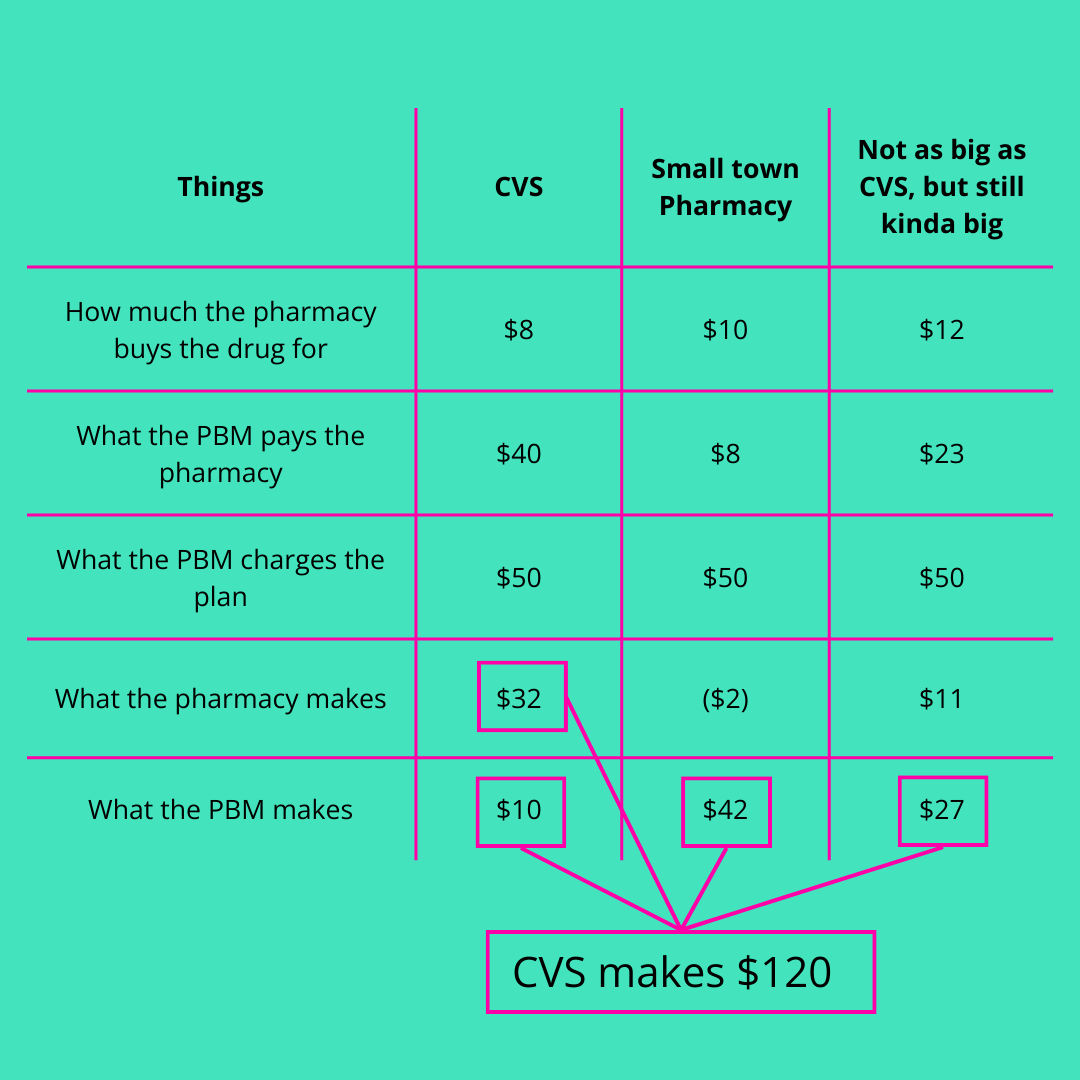
Let’s look at a recent move by CVS to change its pharmacy pricing. While at first glance it seems noble and a step in the right direction, it’s never so simple…
Here’s what the current payment scheme looks like between the PBM and pharmacies:
Here’s what the new one looks like:
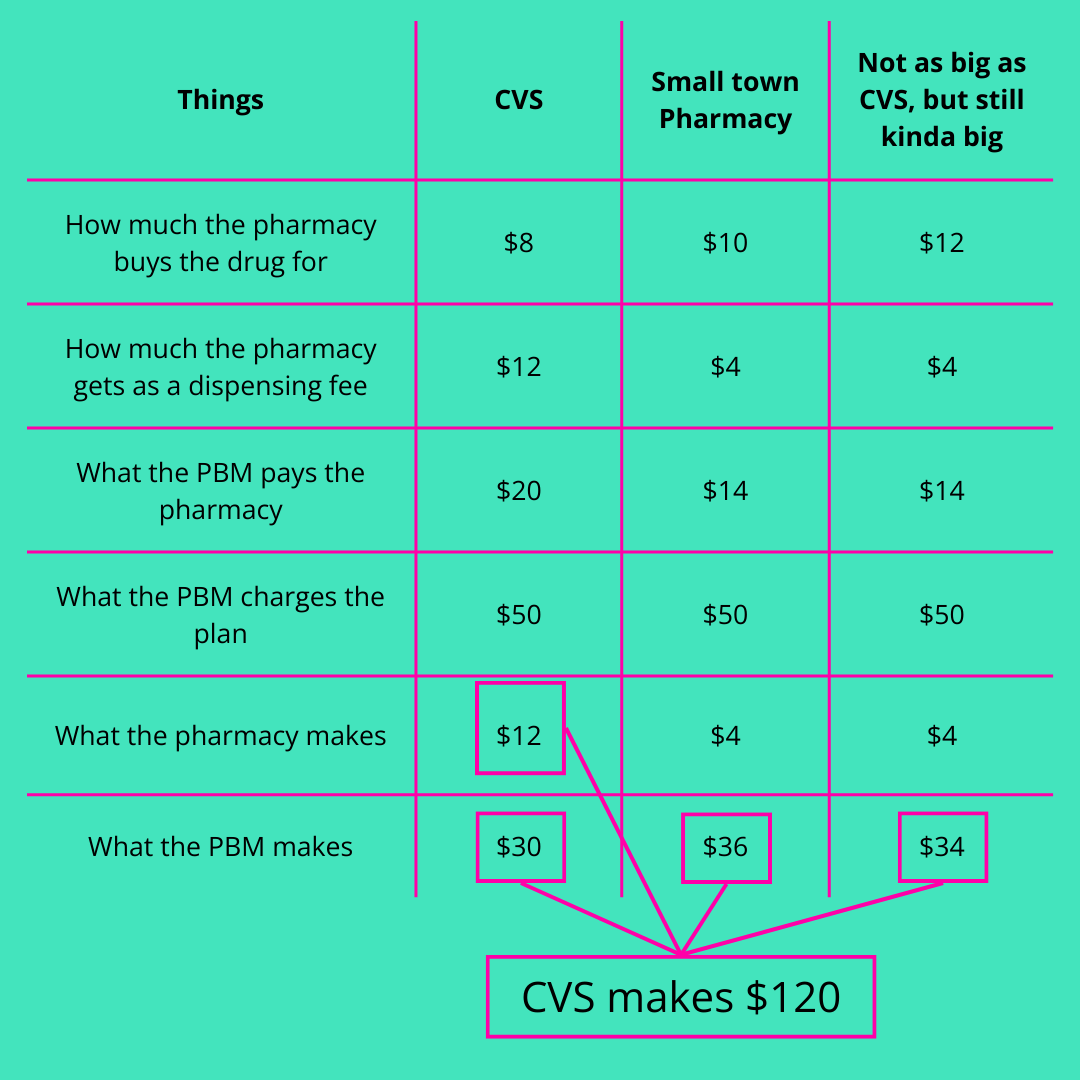
By the way, all credit for these numbers is due to the illustrious Dr. Eric Bricker. To see the true master breakdown this example check out the video here.
You can see that what they’re selling us and to pharmacies is a nice story, a friendly façade, a whole ton of mayo dumped onto chicken… ahem…
In the end, they, you’re friendly neighborhood middleman still make the same amount of money.
Not only that, they are now in a position to redirect patients away from working with the likes of Mark Cuban’s cost plus, whatever thing, or GoodRx.
It’s all just about shifting money around but netting the same amount. And looking better while doing it.
Let’s go again.
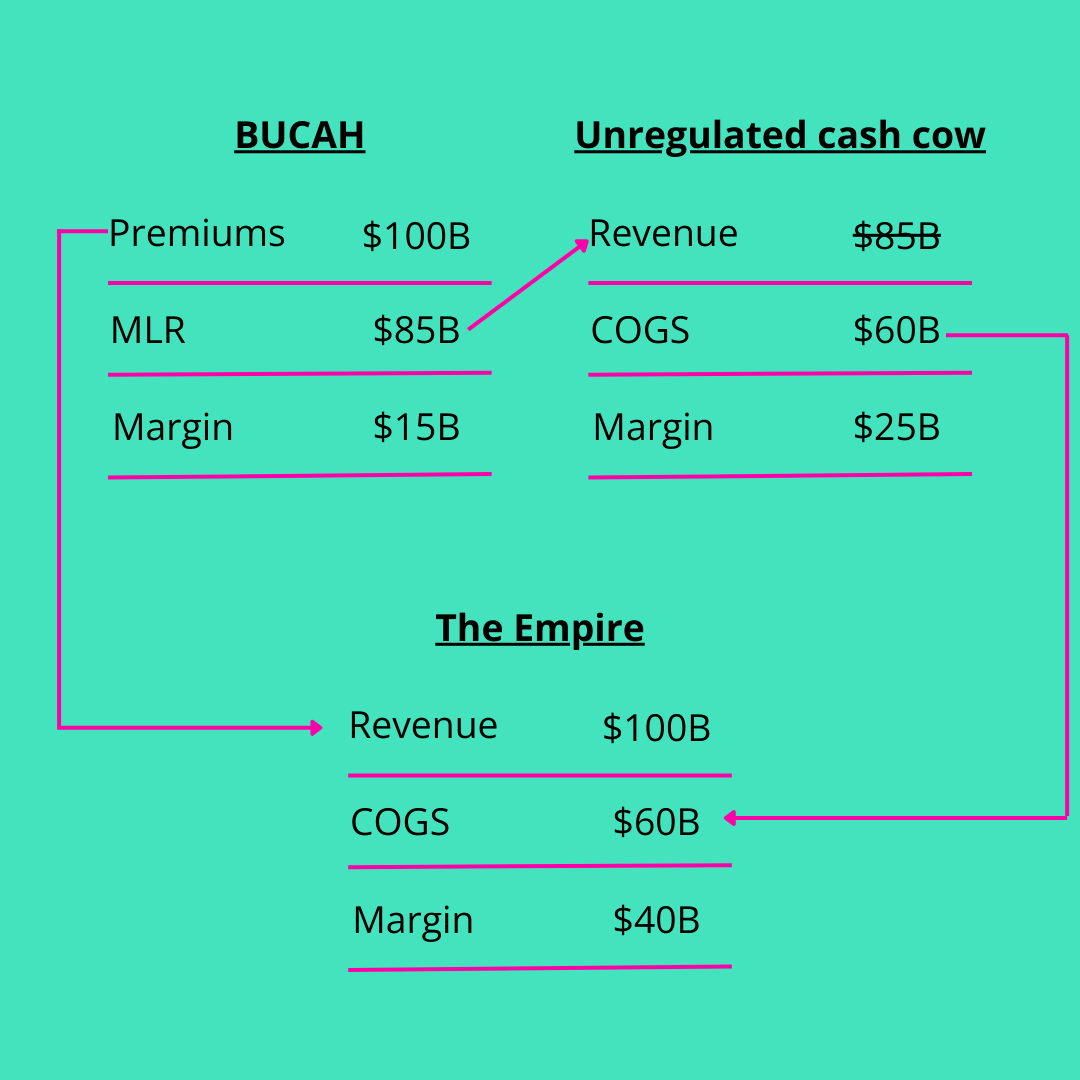
Remember when we did a whole thing on intercompany eliminations? You can read the full breakdown here, but here is the gist.
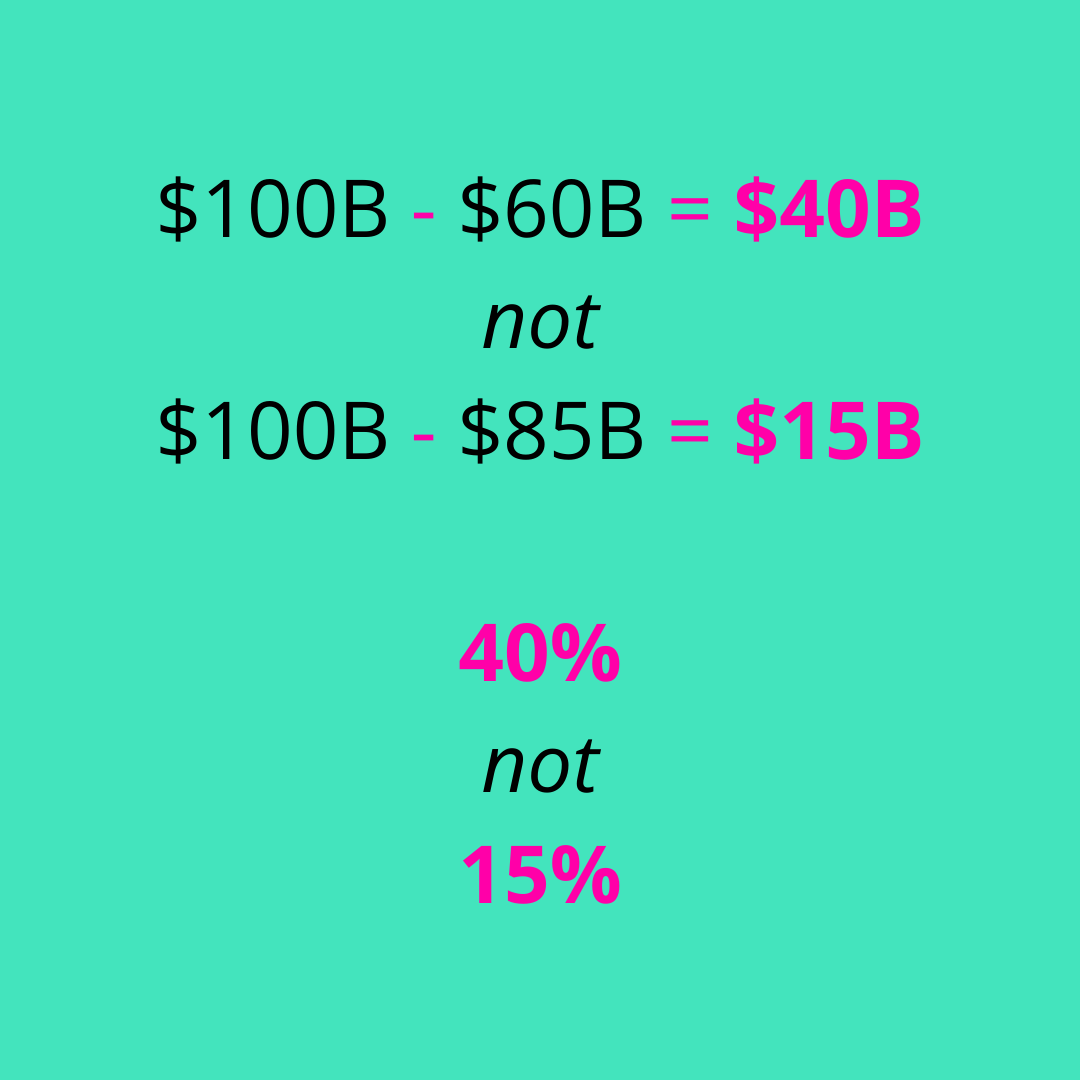
Insurers are not allowed to make more than about 15% in profit. But they sure as heckfire are allowed to buy services at inflated prices from themselves (their subsidiaries) thereby boosting profits in other divisions that are not beholden to medical loss ratios.
Hence the joy that PBMs bring to all insurance companies.
Here’s the example by the numbers:
And not to be outdone, we have to look at pharma companies.
Here’s a great trick they like to play in the game. It’s called copay assistance.
The long and the short is that the drug company makes a drug, something cool like Ozempic. Ever heard of it?
Well, it’s driving up costs almost as much as pickleball. As an aside, every orthopedic practice needs to build a pickleball court in front of their practice. Knees all day.
Or look at a drug like Keytruda. The highest selling drug of all time.
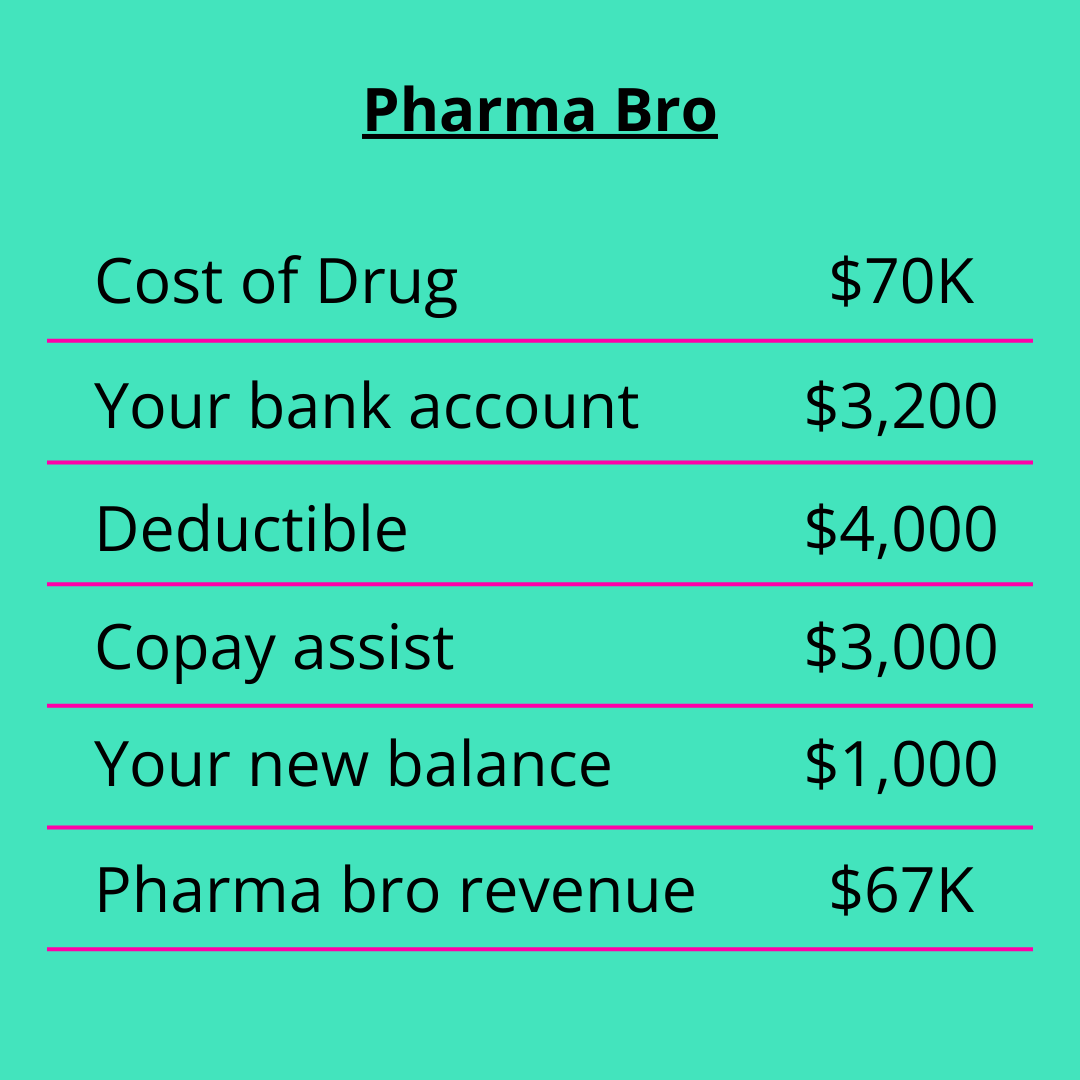
Well, lots of drugs cost lots of money. Say a drug costs, $70,000 per year. You can’t afford that and honestly, you’re $4,000 deductible isn’t too attainable either.
So, Novo Nordisk in its infinite kindness, hooks you up with Copay assist. You get a cool $3,000, which goes towards your deductible.
For simplicity sake, Novo has fronted $3K and made $67K. That $67K gets paid by your insurance plan.
See the game?
Here’s a picture:
I could go on. And I will.
Health Systems. Can’t leave them out.
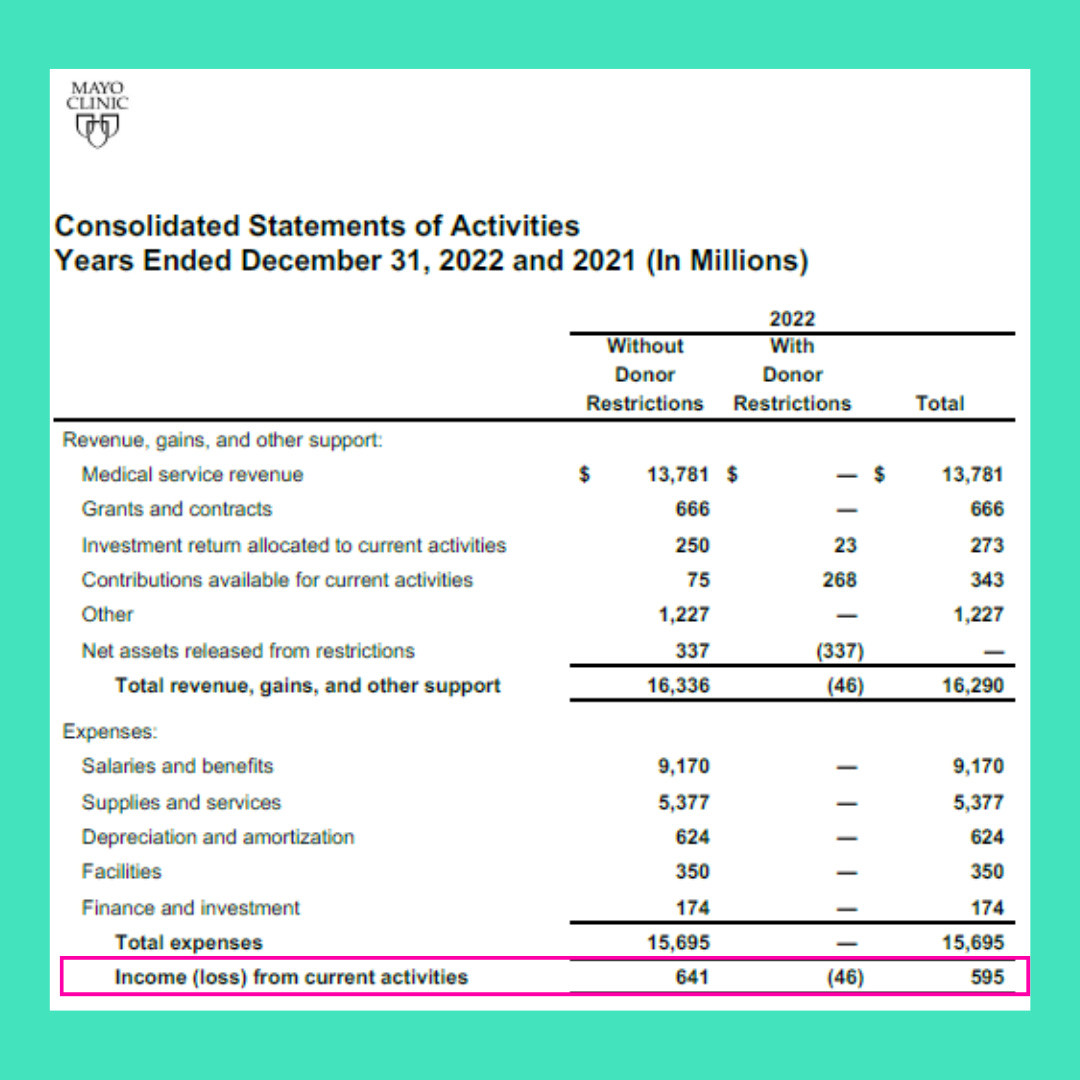
I know, I know. It’s not so easy, headwinds, blah blah. But there’s another side to this tale. Look at certificate of need laws. Look at the asset growth of large health systems. Look at private equity’s involvement in hospitals. HCA, Tenet, CHS. Mayo is in Dubai, while blocking safe staffing legislation in its home state. Cleveland Clinic is in Abu Dhabi.
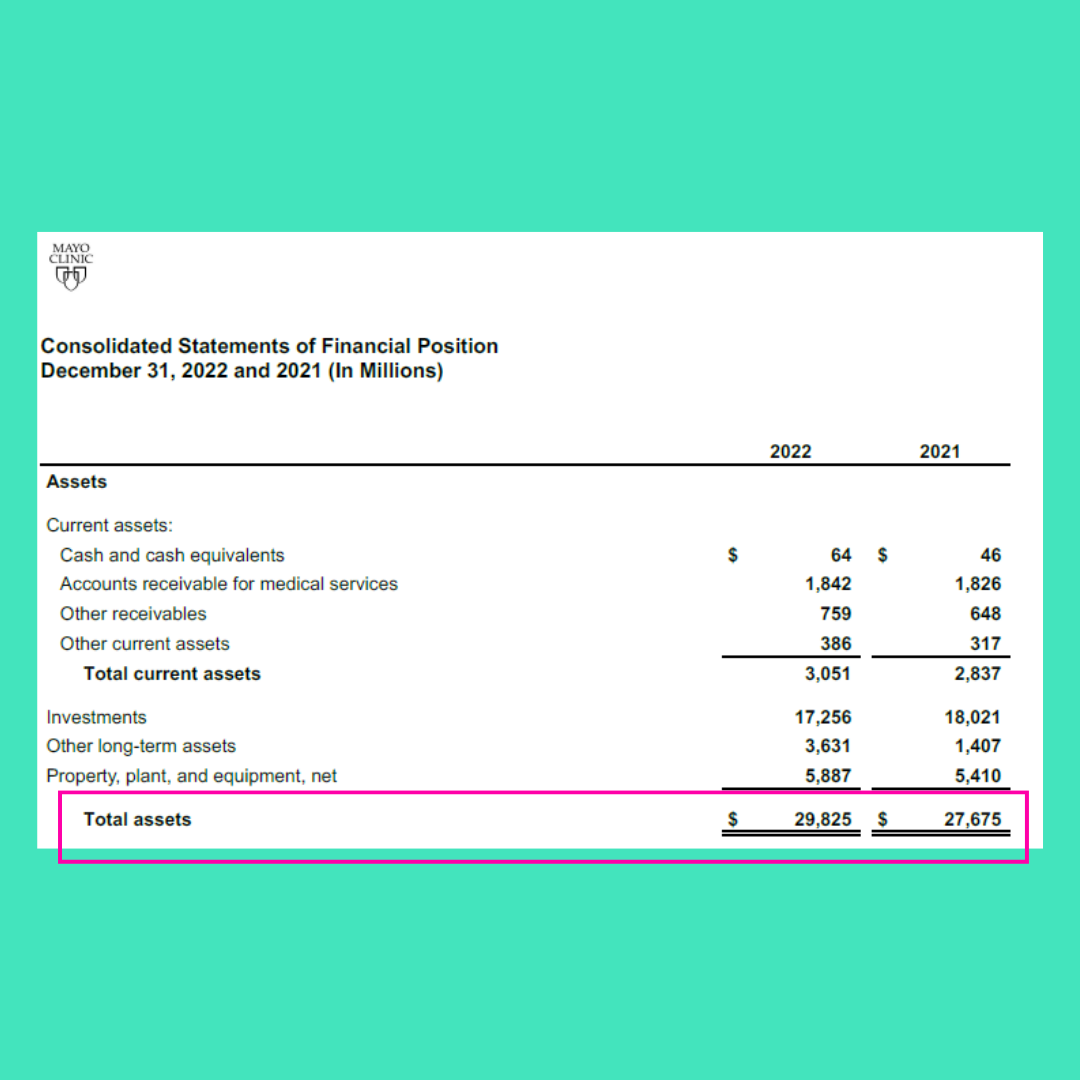
Health systems invest internationally, hide money in the Caymans, invest in hedge funds, private equity, risky REITs, and everything in between.
Y’all, it’s all hiding in plain sight.
Just look at this margin:
Now look at the assets:
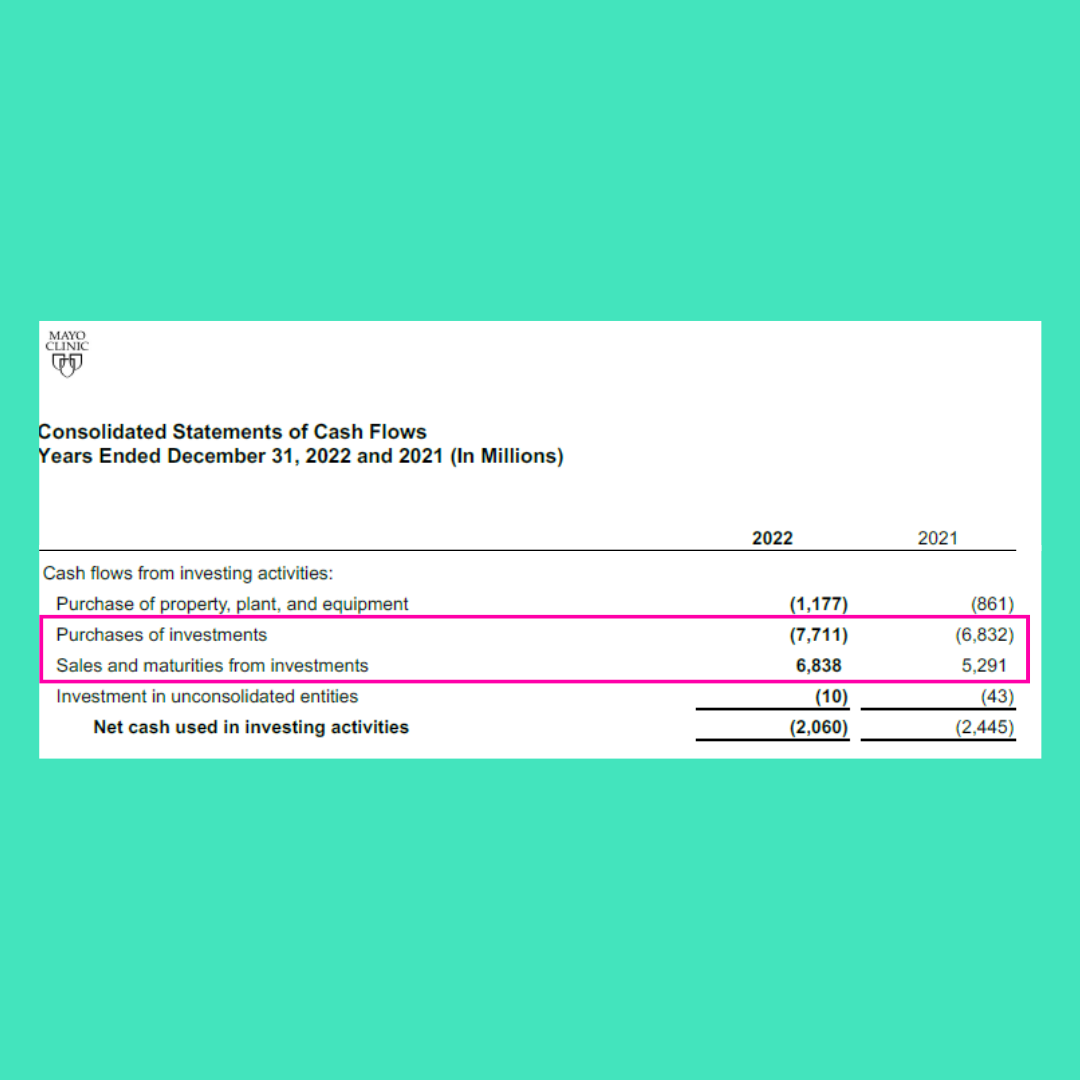
Now look at the cash flow:
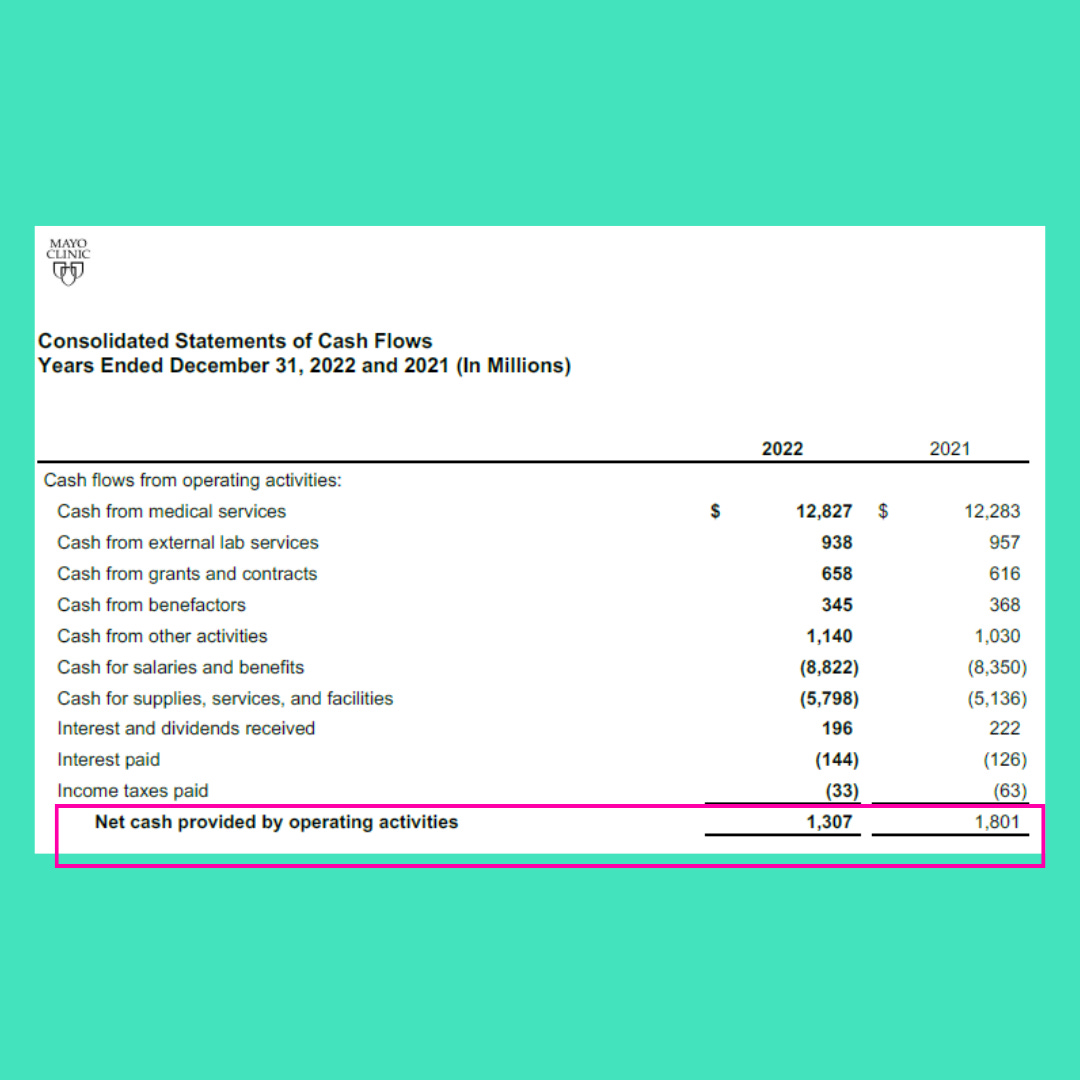
And investments:
It’s all right there. To accomplish this, they dive back into all the policy, contracts, and levers they can.
For example, Certificate of Need laws prevent competition. You need a strong policy arm and relationships to build new facilities, which creates barriers. You can then take advantage of rich markets and get more favorable payor mixes.
And since you have scale, you negotiate with insurers to pay something like 400% of Medicare rates. Maybe more. 1,200% is good too. You also intentionally inflate charity care numbers by making up fanciful charge master numbers to make it look like losses are higher and you have earned your tax exemption.
Horse trading.
It boils down to this. There are very large organizations that will do anything to keep money and power. And while we may wish the government would step in to control costs, the interest there is in jobs.
It’s an unfortunate situation, but it’s the situation.
An ever growing pie fueled by a game of horse.
And not the good kind of pie or the good kind of horse.
Well, now dang, I want some pie and to go play horse.
See you out there!
Very well written. Your illustrations of the PBM game and Pharma "gifts", the MLR ruse and overall GDP/national HC expenditures were very much on-point. I do understand clearly the illustration showed on Mayo Clinic's activities. However, as a seasoned operator of hospitals and health systems, I think attacking the CON as a villain of monopoly-building and price inflation should be tempered with the "why" there was the thought for the laws in the first place. If outpatient competition is(good) for communities wholesale, then how are disparities in access/availability/acuity and regulatory burden addressed now that DSH is eradicated? An example - a local outpatient imaging center opens up across the street from Hernia Memorial Hospital. It has (transparent) prices on outpatient CT, MRI and ultrasound procedures. Let's assume they are 15-20% lower cost to payors/customers than the comparable same examinations at HMH. Steerage from the BUCAHs will occur with lightening speed. So, the YOY OP revenue to HMH will start to wilt. Why is this a problem? It could be that the pricing/revenue differential covered some of the grossly underfunded maternity/critical ICU/ER/Behavioral care that this and most communities manage. We all know what living on CMS-based reimbursements alone does to the futures of hospitals, so I won't bore you. However, the vastly uneven legal (EMTALA), regulatory (State, CMS, etc.) and cost of services (OB, ER, ICU, Trauma) burden that MHM has to fund hour-by-hour needs some funding at a differential for sustainability. I have probably not done the example justice as I am not much of a writer. I only wanted to say that we will need something for whatever we as a country deem as essential services for our communities to be supported. So many more hospitals are just trying to fund their next nursing shift and only serve their local communities, not the UAE. Again, well done.
Preston, this is awesome! I love your writing style and how easily you break down the nonsense complexity we're dealing with in American healthcare. Someday, I'd love to read your thoughts on what everyone seems to be clamoring for -- universal healthcare, medical for all, single payer, or whatever else people are calling it these days. For me, it's the idea that we throw our hands up and say, "we give up" and bend over and let the system have its way with us. I hate it when people say, "every other country in the world does healthcare like this except us". I really need to come up with a better reply but the only one I've come up with to date is "sure, plenty of other countries in the world slaughter their own people with machine guns and chemical weapons but I'm certainly not advocating we copy them on that either". I know, it's not a great comeback. I'm just not a "give up and let the other side win" kind of girl. Anyway, thank you for this great blog. I really like it.